Hello. I’m Dr. Sangmun Choi, Chief Surgeon at Ryan Plastic Surgery Clinic. For those who have been diagnosed with breast cancer and are facing surgery – or for those who know someone going through this – one of the biggest concerns is often, “What will my chest look like after the operation?” Breast reconstruction goes far beyond simply restoring lost volume; it is a profoundly important process that helps heal patients emotionally and guides them back to their everyday lives.
Today’s most common question I hear in consultations: “Where is the best place to put the breast implant?” I’ve brought along a very insightful study to explain this in an easy-to-understand way. The paper we’ll look at today was published in 2019 by Professor Antony’s research team in Plastic and Reconstructive Surgery, one of the world’s most prestigious plastic surgery journals. It explores the evolution of “Breast in a Day” breast reconstruction. I’ll keep the medical jargon to a minimum and explain it as comfortably as I would in my own consultation.
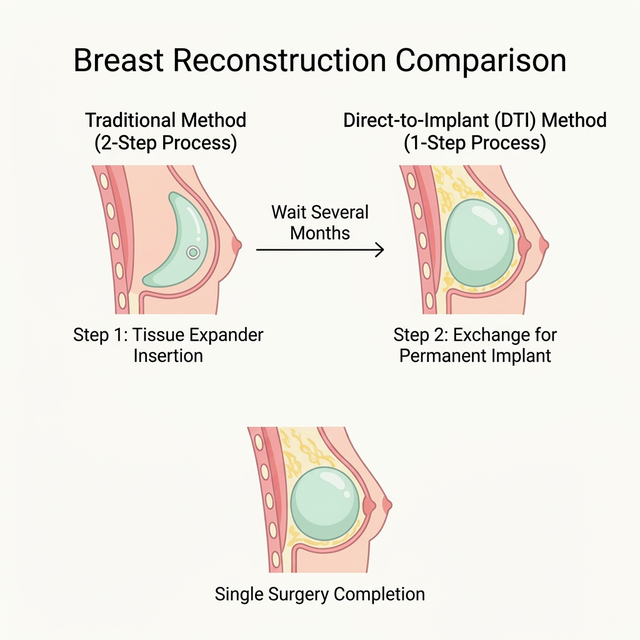
What Was Traditional Reconstruction Like?
In the past, breast reconstruction required a long and arduous journey of patience. After a mastectomy, a device called a “tissue expander” was first inserted to gradually stretch the skin over several months. Then, a second surgery was needed to replace the expander with a permanent implant. For patients, having to go through surgery twice – and living with an expander in between – was an enormous inconvenience.
But medical technology keeps advancing. Recently, Direct-to-Implant (DTI) reconstruction – also known as “Breast in a Day” – has become increasingly popular. This technique completes both the mastectomy and implant placement in a single operation.
Key Question: Under the Muscle or Over It?
The most important topic in this paper – and the one I always make sure to explain to my patients – is implant placement.
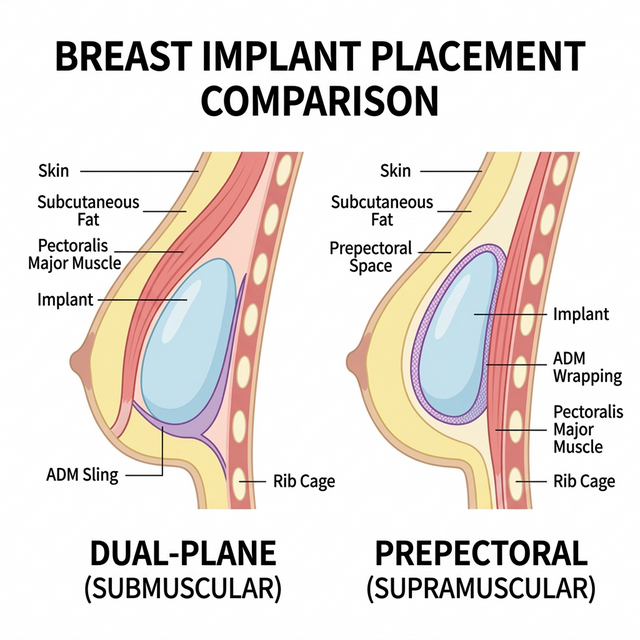
1. Dual-Plane (Submuscular) Placement
In the traditional approach, the implant is placed partially beneath the pectoralis major muscle. While this provides good coverage, it can lead to a well-known complication: animation deformity – visible distortion of the breast when flexing the chest.
2. Prepectoral (Supramuscular) Placement
In the newer prepectoral approach, the implant sits above the muscle, wrapped in an acellular dermal matrix (ADM). This avoids disrupting the chest muscle entirely, eliminating animation deformity and producing a more natural breast shape.
What Did the Study Find?
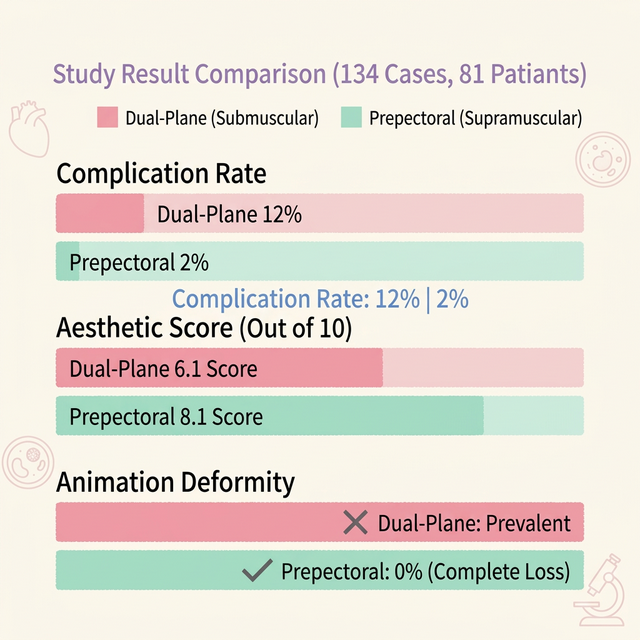
This paper meticulously compared a total of 134 DTI reconstructions performed between 2014 and 2018 – 57 submuscular and 77 prepectoral cases. Four independent physicians who were not involved in the surgeries evaluated the aesthetic outcomes in a blinded fashion, without knowing which patient had received which procedure. The results were both fascinating and encouraging.
Complication Rates Actually Decreased
Surprisingly, placing the implant in the shallower “above the muscle” position resulted in an overall complication rate of just 2%, significantly lower than the 12% rate for submuscular placement. There were zero cases of infection, hematoma, or capsular contracture. This means that in terms of safety – a major concern for many surgeons – the prepectoral approach is by no means inferior, and may in fact be superior.
The Aesthetic Results Were Far More Natural
In blinded evaluations by four physicians, the prepectoral approach scored 8.1 out of 10, dramatically outperforming the submuscular method’s 6.1 points. There was less rippling and less visible show-through of the implant. Most importantly, because the implant sits right where the original breast tissue was, it’s much easier to achieve a beautifully natural, slightly drooping teardrop shape.
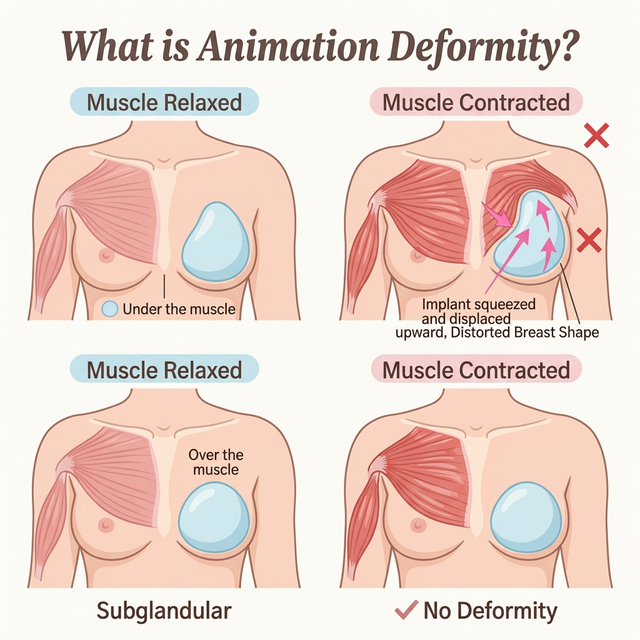
A Complete Farewell to Animation Deformity
This is the result I want to emphasize the most. With the prepectoral approach, there was not a single case of animation deformity – the distortion of the breast when flexing the chest muscles. That’s 0%. Golfers, tennis players – swing away with confidence. Reoperation rates, postoperative pain, and hospital stay duration showed no significant differences between the two methods. The conclusion: it’s safe, pain levels are comparable, and the results are significantly more beautiful and natural.
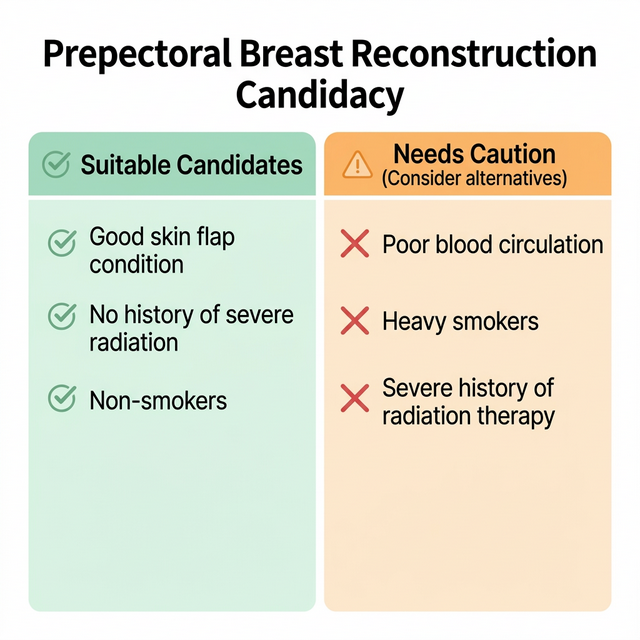
Who Is the Ideal Candidate for Prepectoral Reconstruction?
Not every patient is automatically suited for the prepectoral approach. Adequate skin flap thickness after mastectomy is essential to ensure proper implant coverage and a natural result. During your consultation, your surgeon will assess factors such as skin quality, breast size, and overall health to determine the best option for you.
A Message from the Consultation Room
The message of this study is clear: single-stage prepectoral breast reconstruction is not just a viable alternative – it may represent the new gold standard. Lower complication rates, superior aesthetic outcomes, and zero animation deformity make a compelling case.
If you or someone you love is considering breast reconstruction, I encourage you to have an open conversation with your surgeon about prepectoral placement. Every patient is different, and the best approach is one tailored to your unique anatomy and goals.
If you have any questions, feel free to reach out. I’m always here to help.
Dr. Sangmun Choi
Chief Surgeon, Ryan Plastic Surgery Clinic
Gangnam, Seoul, South Korea